Best Exercises for the Trapezius Muscle
In this article we will discuss the following (click any to jump to that section):
- Scapulothoracic Muscles and Pain
- Biomechanics Review: Scapulothoracic and Glenohumeral Joints
- Anatomy of Trapezius
- From Biomechanics to Exercises
- Choosing the Best Exercise
- [Video] Shoulder Impingement
To start this Evidence-Based Strength Training Series, we’ll take a look at the often-neglected scapulothoracic muscles, their functions and the best exercises to recruit them.
Scapulothoracic Muscles and Pain
Typically, when clinicians consider how to manage upper quarter pain, they’re careful about using local exercise and manual therapy. However, with a proper movement assessment or regional interdependence philosophy, clinicians recognize that impaired scapulothoracic muscles often contribute to pain in distal or proximal joints. Weakness or poor neuromuscular control of the periscapular muscles has been implicated in subacromial impingement4,18, lateral epicondylalgia2,7,12, cervicogenic headache10, and neck pain3,16.
In a prospective cohort study by Clarsen et al, scapular dyskinesis led to an 8.4 times greater risk of shoulder injury during an elite male handball season.6 Further, Lawrence and colleagues found that shoulder pain due to subacromial impingement significantly reduced scapulothoracic upward rotation at lower angles of humerothoracic elevation and sternoclavicular posterior rotation throughout humerothoracic elevation.11
Biomechanics Review: Scapulothoracic and Glenohumeral Joints
- In humeral elevation, the scapula rotates up 1° for every 2° of elevation until 120° are achieved. Afterwards, the scapula rotates 1° for every 1° of elevation until the arm reaches maximal elevation.
- The scapula typically tilts posteriorly between 20° and 40° in the sagittal plane.
- The scapula rotates externally between 15° and 35° in the transverse plane.17
These joint movements rely on coordinated and balanced work from several muscles: the trapezius, serratus anterior, levator scapulae, rhomboid, and pectoralis minor muscles.
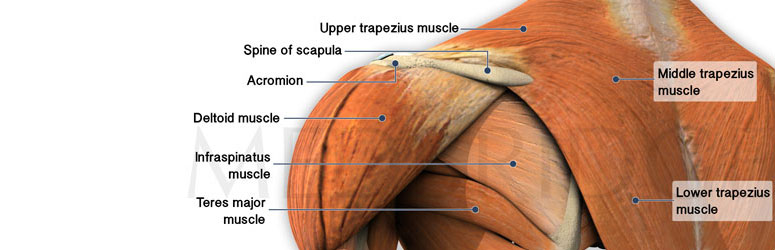
Anatomy of the Trapezius
The trapezius starts at the medial third of superior nuchal line, external occipital protuberance, nuchal ligament, and the spinous processes of C7-T12 vertebrae with a distal insertion at the lateral third of clavicle, acromion process, and spine of scapula.
Trapezius is divided into 3 distinct portions:
- Upper trapezius (UT) providing scapular elevation
- Lower trapezius (LT) providing scapular depression
- Middle trapezius (MT) causing scapular retraction
The UT and LT together rotate the glenoid cavity superiorly, which is often a problem for individuals with shoulder impingement or pain.11
From Biomechanics to Exercises
Upper Trapezius
Primary function: scapular elevation
The highest Maximal Isometric Voluntary Contraction (MVIC) is achieved with elevation of scapula. During scapular abduction, UT activity progressively increases from 0° to 60° and from 120° to 180° of abduction.1
Researchers have found that the highest electromyographical (EMG) activity occurs in the following exercises:
Because UT weakness is rather rare (unless secondary to neurological involvement), it seldom deserves attention when treating the upper quarter pain. Instead, clinicians focus on strengthening middle and lower trapezius and normalizing the activation ratio of UT to the lower two trapezius (MT and LT).

Single Arm Shoulder Shrug

Prone Shoulder Horizontal Abduction
Middle Trapezius
Primary function: scapular retraction
MT is often activated with scapular retraction. The highest MVIC for the MT has been recorded during the following exercises:
As the UT often compensates for a weak MT or LT, it may be beneficial to use exercises with a good UT:MT ratio such as:
- side-lying forward flexion
- side-lying external rotation
- prone shoulder extension5
Lower Trapezius
Primary function: scapular depression
Because LT impacts scapular upward rotation, external rotation, and posterior tilt, its strengthening yields better results than that of UT and MT.17
This connection has been confirmed by many studies of the LT weakness and its association with pain.
Numerous studies also looked into maximal EMG activity of the LT during upper extremity strengthening and determined that MVIC has been significantly higher during the following exercises:
- Arm raised overhead in line with the LT muscle fibers9
- External rotation at 90° of abduction9,15
- Horizontal abduction with external rotation5
- Prone shoulder abduction5
While high MVIC is a good criterion for choosing exercises, an optimal UT:LT ratio can be even better. Being the primary actors in upward scapular rotation, UT and LT should make adequate and relatively equal contributions to maintain normal biomechanics. A study by Cools and colleagues determined that the following exercises have the best UT:LT ratios:
- Side-lying forward flexion
- Side-lying external rotation
- Horizontal abduction with external rotation5
In a similar study by McCabe et al., the following exercises activated the LT over the UT:
- Seated press-up
- Unilateral scapular retraction
- Bilateral shoulder external rotation13

Prone Horizontal Abduction with External Rotation

Prone Lower Trapezius Strengthening
Choosing the Best Exercise
Although these studies give us a glimpse into properly selecting exercise, very few exercises have been or will ever be studied. When choosing an exercise for your patient, be sure to consider:
- the biomechanics of the movement
- current evidence for or against the exercise
- your patient’s presentation, and goals for treatment
The trapezius is an important piece of the puzzle, but the serratus anterior, rhomboids, and levator scapulae also contribute to upper quadrant pain.
For more information on treating shoulder dysfunction, check out Eric Hegedus’s course Evidence-Based Treatment of the Shoulder: An Update.
- Bagg SD, Forrest WJ. Electromyographic study of the scapular rotators during arm abduction in the scapular plane. American Journal of Physical Medicine. 1986; 65: 111-124.
- Bhatt JB. Middle and Lower Trapezius Strengthening for the Management of Lateral Epicondylalgia: A Case Report. Journal of Orthopaedic & Sports Physical Therapy. 2013;43(11):841–847.
- Cagnie B, et al. The Relevance of Scapular Dysfunction in Neck Pain: A Brief Commentary. Journal of Orthopaedic & Sports Physical Therapy. 2014; 44(6): 435–439.
- Cools AM, Declercq GA, Cambier DC, Mahieu NN, Witvrouw EE. Trapezius activity and intramuscular balance during isokinetic exercise in overhead athletes with impingement symptoms. Scandinavian Journal of Medicine & Science in Sports. 2007; 17(1): 25-33.
- Cools AM, Dewitte V, Lanszweert F, et al. Rehabilitation of Scapular Muscle Balance: Which Exercises to Prescribe? American Journal of Sports Medicine. 2007; 35(10): 1744–1751.
- Clarsen B, Bahr R, Andersson SH, Munk R, Myklebust G. Reduced glenohumeral rotation, external rotation weakness and scapular dyskinesis are risk factors for shoulder injuries among elite male handball players: a prospective cohort study. British Journal of Sports Medicine. 2014; 48: 1327-1333. doi:10.1136/bjsports-2014-093702.
- Day JM, et al. Scapular Muscle Performance in Individuals With Lateral Epicondylalgia. Journal of Orthopaedic & Sports Physical Therapy. 2015. [Epub ahead of print]
- Decker MJ, Hintermeister RA, Faber KJ, Hawkins RJ. Serratus Anterior Muscle Activity During Selected Rehabilitation Exercises. American Journal of Sports Medicine. 1999; 27(6): 784–791.
- Ekstrom RA, Donatelli RA, Soderberg GL. Surface Electromyographic Analysis of Exercises for the Trapezius and Serratus Anterior Muscles. Journal of Orthopaedic & Sports Physical Therapy. 2003; 33(5): 247–258.
- Jull G, Barrett C, Magee R, Ho P. Further clinical clarification of the muscle dysfunction in cervical headache. Cephalalgia. 1999; 19(3): 179-85.
- Lawrence RL, Braman JP, LaPrade RF, Ludewig PM. Comparison of 3-Dimensional Shoulder Complex Kinematics in Individuals With and Without Shoulder Pain, Part 1: Sternoclavicular, Acromioclavicular, and Scapulothoracic Joints. Journal of Orthopaedic & Sports Physical Therapy. 2014; 44(9): 636–A8. doi:10.2519/jospt.2014.5339.
- Lucado AM, Kolber MJ, Cheng MS, Echternach JL Sr. Upper Extremity Strength Characteristics in Female Recreational Tennis Players With and Without Lateral Epicondylalgia. Journal of Orthopaedic & Sports Physical Therapy. 2012; 42(12): 1025–1031. doi:10.2519/jospt.2012.4095.
- McCabe RA. Surface electromyographic analysis of the lower trapezius muscle during exercises performed below ninety degrees of shoulder elevation in healthy subjects. North Amican Journal of Sports Physical Therapy. 2007; 2(1): 34-43.
- Moseley JB. EMG analysis of the scapular muscles during a shoulder rehabilitation program. American Journal of Sports Medicine. 1992; 20(2): 128–134.
- Myers JB, Pasquale MR, Laudner KG, Sell TC, Bradley JP, Lephart SM. On-the-Field Resistance-Tubing Exercises for Throwers: An Electromyographic Analysis. Journal of Athletic Training. 2005; 40(1): 15–22.
- Petersen SM, Wyatt SN. Lower Trapezius Muscle Strength in Individuals With Unilateral Neck Pain. Journal of Orthopaedic & Sports Physical Therapy. 2011;41(4):260–265. doi:10.2519/jospt.2011.3503.
- Reinold MM. Current Concepts in the Scientific and Clinical Rationale Behind Exercises for Glenohumeral and Scapulothoracic Musculature. Journal of Orthopaedic & Sports Physical Therapy. 2009; 39(2): 105–105.
- Schmitt L, et al. Role of Scapular Stabilizers in Etiology and Treatment of Impingement Syndrome. Journal of Orthopaedic & Sports Physical Therapy. 1999; 29(1): 31–38.

